Event Description
I’m a Frontline Facility – How Can I Safely Test Clinical Specimens From a Suspected Ebola Patient

Description:
Join us for our next OneLab™ Network Event in which will give an overview of the current Sudan Ebolavirus outbreak and discuss testing options for frontline facilities, identifying potential hazards in laboratory processes, and risk mitigation strategies for safe laboratory testing.
Event Speakers
Keynote Speakers

Nancy Cornish, M.D., PhD
Medical Officer, Senior Advisor for Quality and Safety
Division of Laboratory Systems (DLS)
Center for Surveillance, Epidemiology and Laboratory Services (CSELS)
Office of Public Health Scientific Services
Centers for Disease Control and Prevention (CDC

Vicki Herrera, MS
Research Coordinator
Infectious Diseases and Bioaerosols NETEC
Laboratory Working Group Lead
University of Nebraska Medical Center

Brian H. Harcourt, PhD
Biosafety Officer
Viral Special Pathogens Branch
National Center for Emerging and Zoonotic Diseases
Centers for Disease Control and Prevention
Event Media
Event Media
Audio Transcript
Date of session: 11/17/2022
CHELSEA PARSONS: Hello, everyone. Thank you so much for joining, for hopping on here early. We’re excited to get started. We’re going to give everyone just another minute to join on. And we’ll go ahead and start then. Thanks again.
Hello, everyone. Welcome again. Thank you so much for joining today. We’re very excited to get started with our OneLab™ Network event, “I’m a Frontline Facility– How Can I Safely Test Clinical Specimens from a Suspected Ebola Patient?”
So before we get started, I’m just going to walk through a couple housekeeping items. If you’re having any technical issues before we get started, you can please feel free to send those to onelab@cdc.gov. That’s onelab@cdc.gov. You’ll see that was just posted in the chat here.
Any technical issues throughout, please feel free to email us there. If you have questions related to the session, throughout the session, please feel free to drop those in the Q&A function. You’ll see it in the banner at the bottom of your screen. It’s the Zoom Q&A function. You can post those throughout the whole event.
We’re going to have a designated Q&A session at the very end of the presentation where we’ll try to get to as many of those questions as we can. Do not fear if we don’t get to your question today. We will do our best to answer them via email following the event. If any questions come up after the event, you can also email that OneLab™ inbox to shoot your questions our way. That’s onelab@cdc.gov.
Please note that we posted in the chat the link for closed captions. If you need closed captions, throughout this event, open up that link. Put in that code. And you’ll just need to keep that link open as well as this Zoom event for the entirety of the event.
All right, let’s take a look at our agenda for today. Today, we’re going to get started by talking about a few OneLab™ resources that are relevant to today’s topic. We’ll introduce our presenters and our moderator for this session. We’ll get into the main presentation.
We’ll have that short Q&A session like I mentioned. And then we’re going to introduce our upcoming December OneLab™ Network event. So now I’d like to turn it over to our OneLab™ Network lead, Alicia Branch, to share some of our new and relevant resources. Thanks, Alicia.
ALICIA BRANCH: Thanks, Chelsea. Before the main presentation, I would like to take a moment to share some of those helpful OneLab™ Network resources related to today’s presentation. First, we want to highlight the “Introduction to Laboratory Risk Management” e-learning course, which provides an overview of the basics and the importance of risk management in a laboratory.
Next is the “Fundamentals of Working Safely in a Biological Safety Cabinet”– or BSC– e-learning course. And we also have an interactive virtual reality course. All the links have been provided in the Zoom chat. Next slide, please.
I want to remind everyone that the slide deck may contain materials from panelists not affiliated with CDC. In addition, presentation content from external panelists may not necessarily reflect CDC’s official position. Next slide, please.
And today’s moderator is Dr. Nancy Cornish. Dr. Cornish is a physician, pathologist, and clinical microbiologist. She earned a BA in philosophy from the University of Vermont and a doctor of medicine as well as completed her pathology residency at the University of Vermont School of Medicine.
After completing a fellowship in clinical microbiology at the Cleveland Clinic Foundation, Dr. Cornish went on to serve as the director of the clinical microbiology department at the Cleveland Clinic and then as a general pathologist and director of clinical microbiology at Nebraska Methodist Hospital in Omaha, Nebraska.
Now she serves as a medical officer and the senior advisor for quality and safety at CDC in the Division of Laboratory Systems. Your moderator for today is Dr. Nancy Cornish. Nancy, are you on mute?
NANCY CORNISH: Good morning, everyone. I would like to now introduce you to Ms. Vicky Herrera. Ms. Herrera has worked in the clinical laboratory for the past 18 years. She worked in the Nebraska Public Health Laboratory for nine years as the supervisor in molecular microbiology and the LRN sections.
She is currently working as the research coordinator at the University of Nebraska Medical Center in the field of infectious diseases and bioaerosols. She has supported the Nebraska Biocontainment Unit for the last 13 years and currently supports both NETEC and the Nebraska Biocontainment Unit laboratory by providing education and training to laboratory staff. In addition, she is the alternate responsible official for the University of Nebraska Medical Center Select Agent Program.
I would also like to introduce you to Dr. Brian Harcourt, who will be assisting with our Q&A session he is a biosafety expert and is joining us from the Ebola response that is occurring in Uganda right now. So he is representing CDC in Uganda. Before Vicki goes to our main presentation, I would like to turn it over to Mr. Benjamin Mattson of the University of Nebraska Medical Center to talk about the CEUs offered for today’s section. Mattson?
BENJAMIN MATTSON: Thank you, Nancy. Good morning. Good afternoon, everyone. My name is Benjamin Mattson. And I’m representing NETEC and the University of Nebraska Medical Center today.
I’m an instructional designer with the NETEC grant. And I am housed at UNMC. The University of Nebraska Medical Center’s Center for Continuing Education is assisting and facilitating continuing education units for today’s webinar.
We’ll get started shortly with just some brief information about the CEs and then an introduction to NETEC. And then we’ll bring Vicki on. The objectives for today’s webinar will be discussing frontline facilities’ clinical testing options, identifying potential hazards in laboratory processes, and discussing risk mitigation strategies for safe lab testing.
The activity today has been accredited for one hour of continuing education for nurses’ CNE, physicians’ CME, and laboratorians’ P.A.C.E.®. One credit is available. We have some instructions here for P.A.C.E.® on the bottom of this slide. But rest assured, we have additional instructions waiting for you for all those seeking CEs.
Here is the UNMC Center for Continuing Education’s disclosure declaration, making it available today. And here is a list of the planning committee and faculty for today’s presentation. Now in order to obtain your CEs for this webinar, we just have a few things for you to do. Number 1, you need to attend the entire webinar today.
At the conclusion of the presentation today when we sign off, you’ll have an opportunity to take a SurveyMonkey survey. There’ll be a link that’s generated at the conclusion of the webinar in Zoom for you to click to access that survey. We need you to complete that survey. You’ll have 10 days to do so.
In the follow-up email after your attendance today at the webinar, we will have additional instructions for how you can obtain your CE certificates after you complete that evaluation. It’s going to include accessing instructions in this post-webinar email and then copying a code for CNE/CME as well as a link, code, and identifier for a CE for P.A.C.E.® in the CE portal.
Now there will be several opportunities for you to ask for help, too. If you do get stuck, we want to go blanketly say if you have a question, run into an issue, need assistance with your CE certificates after today’s webinar, please don’t hesitate to reach out and contact NETEC at info@netec.org. And we’ll be ready to assist.
You may see a screen like this on your machine at the end of the webinar today when it closes. That opportunity to take that survey should be right there. You can click a blue Continue button. And you’ll be able to walk right into that survey.
Additionally, a link to that survey will be sent out in a post-webinar email. And you’ll have 10 days to complete that survey. Any additional assistance you need, don’t hesitate to reach out and contact NETEC, info@netec.org.
I’d like to provide just a bit of introductory information for those of you who may not be familiar with NETEC. This is the NETEC mission statement here on the screen. NETEC sets and advances the gold standard for special pathogen preparedness and response across health care delivery systems with the goals of driving best practices, closing knowledge gaps, and developing innovative resources.
And NETEC tech accomplishes this in a few different ways. We do have four areas of focus. There are only three on the screen described here. But we’ll get to the fourth in just a moment.
We have a consultation effort at NETEC, an education and a research effort, of course. Through the consultation effort at NETEC, we provide opportunities for facilities’ self-assessment, collection and sharing of metrics, onsite assessments, guidance. And NETEC provides emergency on-call mobilization for facilities as needed.
That’s the consultation effort of NETEC. We have an education arm of NETEC, which I’m involved with as a designer. We offer in-person training courses.
We have an online repository of online courses and information. We have a NETEC resource library full of references, tools, resources ready for you, which we can find after the webinar today by navigating to our website, netec.org. Now that is free and open for you to access– contains links to all the resources that NETEC has been curating, including exercise templates, one of the more popular options, available free of charge in that online repository.
The research arm or focus of NETEC is busy establishing central IRB processes, working on policies and procedures, working with facilities who conduct research, including helping create the infrastructure for a specimen biorepository. Those are the three main areas that NETEC focuses on. And the fourth one, which has been in action for quite a while, is an international outreach that NETEC is working with.
NETEC partners closely with biocontainment experts internationally. We provide assistance, guidance, hands-on help if needed for facilities looking to develop best practices, work on procedures, and develop some of that international strategy in biocontainment. So that’s the fourth arm, the international outreach arm of NETEC.
And at this time, I’ll say– we’ll introduce Vicki, of course, for her presentation. Additional information on CEs will be available, instructions after the webinar in that post-webinar email. And I’ll just stress once again, if you have any questions about today’s presentation or about obtaining those CE certificates, please feel free to reach us at info@netec.org. And now I’ll turn the presentation over to Vicki.
VICKI HERRERA: Great. Thank you, Benjamin. And thank you all for joining me today, allowing me to speak on this topic that’s very near and dear to my heart. Next slide, please.
So today, we’re going to discuss frontline facilities’ clinical testing options, identify potential hazards in laboratory processes, discuss some risk mitigation strategies for the laboratory testing. So we’re first going to talk about what’s going on with the outbreak. We’re going to go over some risk assessment, mitigating the risks, and a few other considerations. Next slide, please.
OK, the current Sudan virus outbreak– next slide, please. September 20 was the first confirmed Ebola virus disease outbreak caused by Sudan virus in Uganda. So it has been almost two months since this outbreak was first identified. And as of November 15, that outbreak has spread to nine different districts.
The confirmed cases right now, this is probably changing. But the latest case counts that we had access to were 140 confirmed cases, with 55 deaths that are confirmed. There are also some probable cases within those numbers.
So again, the numbers are continuing to change. But what I want to point out here is that there has been 18 health care workers that have been infected, with seven deaths. And this is one of the reasons why we do what we do at NETEC. We want to help prevent as many of those infections as we can. Next slide, please.
So currently, the CDC has issued a level 2 alert for this area. This means that US health care workers should remain vigilant and screen patients with compatible symptoms, exposures, and recent travel history. Health care facilities should implement, identify, isolate, inform processes for early and rapid patient identification.
And health care facilities should review their special pathogens preparedness plans. So that’s what we’re going to talk about today is the laboratories plan. Next slide, please.
So first, we’re going to talk about risk assessment. The basics of a special pathogen preparedness plan must include a risk assessment. But before we even get to the risk assessment, what does it mean to be a frontline facility? So who are the frontline facilities? You may have heard about the tiered structures across the nation with treatment centers, assessment hospitals, and frontline hospitals.
But technically, everyone is a frontline, regardless of this designation. A frontline facility is the first line of identification for a patient that may have a special pathogen. These patients could walk into any care facility across the nation, which means the size of the frontline could greatly vary from a two-bed hospital in rural central Nebraska to a 1,000-plus bed in the middle of New York City.
So what are the expectations of a frontline? So currently, the guidance reads that regardless of size, clinical laboratories should be prepared to provide a timely and minimum menu of testing to ensure that medical evaluation is not delayed for any patient. Frontline health care facilities are not expected to provide prolonged care for more than 24 hours for a severely ill patient.
But is that a reasonable expectation? Right, it really depends. It may be for some but not for others. What if? There are so many “what ifs” that we could address here.
But what if you’re a small, rural hospital and there are no treatment or assessment hospitals that are nearby? And I’ll add, for those of you in cold states, there’s a snowstorm. And the roads are closed. You can’t move that patient out of your facility. That may seem like a far-fetched scenario for some of you.
But think about the possibility that you may have to care for a patient that needs laboratory testing for longer than 24 hours. You may have to wait longer than that just to get a diagnostic test back, depending on where you’re located at or where your closest Ebola testing lab is located. So even though the guidance says that you only need to care for them for 12 to 24 hours, that may not be the reality of your situation, so next slide.
So what are some test menu considerations? So let’s say that you do have to care for that patient longer than that. And they do require some laboratory tests. Next slide.
So these are currently the recommended tests for patient care and management of an Ebola patient. But can your facility really perform these tests– CBCs, basic electrolytes, liver functions, coag testing, urinalysis, blood cultures, malaria testing, influenza testing? And this slide is a little bit behind.
Because we now have a huge surge in RSV. COVID is also there. So respiratory testing might be on the differential, depending on where you’re at and what’s circulating at the time. Next slide, please.
So before we even get to the risk assessment, there are some questions that you can ask. So what testing does your facility currently even offer? Do you have any point of care devices? Do you have automated systems?
Again, this may be very different, depending on the size of your facility. Have you discussed any of this with your care teams? What tests are expected if you were to get somebody to walk through your doors? What are on the must-have list? And what are on the wish list items?
These are two very different things. And they may vary when we’re talking about specimens that could contain special pathogens. So communications with your care teams, and your leadership, your laboratory personnel, these are all very key. Next slide, please.
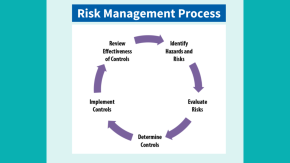
And first, I want to reassure you that routine laboratory testing can and has been done successfully and safely on patients with special pathogens. However, these specimens should be treated with caution. And safety measures should be taken in order to keep you and your laboratory staff safe. You’ve probably seen some variation of this risk assessment or risk management process. But in general, you want to identify the hazards or the risks.
You want to evaluate those risks. You want to determine what controls you can take to mitigate those risks. You want to implement those controls. And then you want to review everything for effectiveness of those controls. And next slide, please.
So what are some of the risks that you can encounter when doing patient testing? Keep in mind this is not an all-inclusive list. But there are some risks that you’ll find just in your typical laboratory settings. I mean, you could have open tubes, centrifugation, sharps, leaky specimens– everybody’s favorites– performing smears, spills, fixing slides, slide agglutination.
What if you don’t have a biosafety cabinet? Working alone, how about allergy to latex? There’s some very obvious ones on here and maybe some not-so-obvious ones. Next slide, please.
Once you’ve identified your risk, you want to evaluate that risk. The infectious dose of Ebola is very low. Therefore, many of the risks identified in the laboratory could be in the high or extreme category.
For example, a leaky tube that’s not in a secondary container could expose you to bodily fluids and would therefore present an extreme risk. Next slide, please. So once you’ve identified that risk, how are we going to mitigate the risks? So next slide, please.
We need to control the risks. And there’s lots of different ways to do this. But just keep in mind that your safety is just as important as the patient’s safety. Next slide, please.
So this is a schematic of the hierarchy of controls that you’ve probably seen before. We’re going to focus on the bottom three, which include PPE, administrative controls, and engineering controls. Next slide, please. So first, we’re going to talk about personal protective equipment, or your PPE. Next slide, please.
The PPE is very important. Even though it’s the lowest on the hierarchy of controls, if you don’t have other controls in place, then PPE becomes very important. So in determining the appropriate PPE, it’s important to know what virus or disease you may be working with.
As laboratorians, we may not always know that information. We hope that, if there’s a person under investigation, that communication with the lab would happen. And I always encourage overcommunication with the laboratory leadership and personnel by the care team.
NETEC has put together a matrix in here to help you determine the most appropriate PPE to use, depending on the virus or disease you may be dealing with. So again, it is very important for the care team to communicate with the laboratory if they are suspecting something that is a high consequence pathogen in their patient. Next slide, please.
So what is the difference between viral hemorrhagic PPE and why? Again, because the infectious dose for Ebola and other viral hemorrhagic fevers is very small, the amount of virus present in many bodily fluids is very large. And therefore, full body coverage of PPE is recommended.
The PPE selection should consider tasks that are to be performed. How close or prolonged contact will you have? What’s the potential exposures to body fluids? And in the laboratory, that’s a great, great exposure risk– and contaminated items that may be on surfaces in other areas.
Patients’ conditions may change and could rapidly and subtly present with bodily fluid risks. And you should anticipate that. Now that may seem like that’s not important to the laboratory. But consider those that go in to do collections.
The use of a trained observer should be considered. Trained observer would be the same as a buddy. So consider the tasks that you’re doing such as verifying that you have correctly donned all of your PPE, observing you as you’re doing those tasks, specimen collection, waste handling procedures, anything that you may be doing in the laboratory.
Keep in mind that donning complex ensembles takes time. So you need to plan for that time. Once you’re appropriately donned, take care to avoid contamination of the PPE and the patient– if you’re in the room, the patient care environments.
Not all PPE is amenable to being cleaned while it’s in use. So keep that in mind. And contamination on the PPE, skin, or clothing may not be visible.
So trained observers or partners should monitor for inadvertent contamination during the use and doffing of PPE. Regardless of your task, consider the PPE contaminated. And doff with care. This is very important. Next slide, please.
So what PPE should you use if you have an Ebola patient? This may vary depending on your facility. There is recommended PPE when there’s potential for bodily fluid exposure. And again, keep in mind that, if you are the one that needs to go in and collect specimens, that this may be your better ensemble.
If you are in the laboratory, it may differ a little bit. And given the recent PPE shortages, it may depend on what you have available in your facility. Next slide, please.
So CDC and NETEC have a lot of informational resources regarding PPE. It’s important to look at what you have on hand. And see what makes sense for the tasks that you are doing. This is a NETEC-provided schematic of some of the different types of PPEs and what you can use. Next slide, please.
Next, we’re going to talk about engineering controls. And then we’ll come back to administrative controls. But engineering controls reduce or prevent hazards from coming in contact with workers.
Engineering controls can include modifying equipment or the workspace, using protective barriers, ventilation, and other things. So we’re going to walk through a few of the risks and how you can utilize engineering controls to protect yourself. Next slide, please.
A biosafety cabinet is one engineering control that is such a great asset to laboratories. When it is used correctly, biosafety cabinets can help protect personnel. But not all laboratories have one.
Not everyone uses them correctly. The CDC, as mentioned earlier, has a great resource on the basics of how to use the biosafety cabinet. And the link is in both the beginning and the end of the presentation.
NETEC also has a video that will link at the end that shows you how to work safely in the biosafety cabinets. But you want to make sure that you are minimizing the items that are inside the cabinet. You also want to make sure that you’re not blocking the airflow vents.
So this is going to limit you on the amount of instrumentation or other items that you can have inside the cabinet. You should also minimize your movements in order to maximize the efficiency of the cabinet. Next slide, please.
All right, let’s talk about some different risks, scenarios, and how we can mitigate those. So specimen collection, there are many risks that you can identify associated with specimen collection. There’s needles, other sharps involved, direct contact with the patient.
So how would you mitigate some of those risks? And this is, again, not an all-inclusive list. This doesn’t identify all the risks involved with specimen collection. But some simple things that you can do that will help reduce your risk is maybe considering the hand placement when drawing a blood sample.
You want to make sure that you’re not anchoring above the needle. Appropriate PPE when you’re in the room with a patient– absorbent pads, you can put an absorbent pad both underneath the arm or wherever you’re drawing your labs. You can use that to put against your PPE to help as a barrier.
Making sure that you have sharps containers and appropriate containers nearby; making sure that you have all of your collection supplies with you so that you don’t need to enter and exit the room; making sure that you have safety devices that are available when collecting– again, this is not an all-inclusive list but just something to consider as you’re critically thinking through the steps on how you would mitigate these risks. Next slide, please.
What if you need to open a tube? Some people have automated systems that are closed tube. But what if you don’t? What if you need to open a tube there?
So how are you going to mitigate those risks? Again, thinking through all of the processes that go into opening a tube– so selecting the right PPE again. That’s going to be your first line of defense.
If you have a biosafety cabinet, that’s fantastic. Use those. Use the biosafety cabinet to open your– sorry. Put your specimen in the biosafety cabinet when opening.
Absorbent pads, there’s examples here, absorbent pads you can use to open the tubes. This will help prevent contamination on your gloves. It also makes the potential contamination easier to see– and again, maybe utilizing point of care instrumentation that could be put in a biosafety cabinet versus putting something on an automated system. All right. Next slide, please.
But what if you don’t have a biosafety cabinet? How could you mitigate risks, again, if you need to open a tube or if you have to use a point of care device? Could you use a shield, for example?
How about just separating a room for your testing, having a separate room, eliminating traffic in that area? Would you have access to a class III glove box– again, different things that you can think through carefully that you could utilize in your lab. Next slide, please.
Aerosolization, that’s kind of a big one in the laboratory. We know that centrifugation is known to produce aerosols. So how could you mitigate that?
If, again, if you have a biosafety cabinet, maybe you could centrifuge in there, depending on how big your centrifuge is. Using closed rotors is something that should be used if possible. If that’s not available, maybe there’s a shield that you could use to put over the centrifuge.
Maybe you could wait a longer period of time before you open the centrifuge cabinet– so again, just thinking through those processes one by one and seeing if there is something that you can do to mitigate those risks. If you can’t mitigate that risk, maybe the test that requires centrifugation is not an option. Maybe you need to look into a point of care device or something else that you could use to provide that type of testing. Next slide, please.
How about a leaky sample? Oh, that’s always the favorite in the lab. This is one of the items that the laboratory just loves to see. So what can you do in this situation? Could you ask them to redraw the specimen?
There’s a lot of things that you have to think about if a redraw is necessary. That’s also providing another needle stick for a patient. You have laboratory staff or you have nursing staff going back into the room with a patient.
So really consider if that’s an option. And if that’s not, could you use a bag to hold the specimen and then carefully place it on an absorbent pad– again, making sure that you have appropriate PPE. If you have a biosafety cabinet, again, that’s going to be one of your best defenses in the situation.
But perhaps you can put it on a absorbent pad. And then you can use an EPA-approved wipe to pick up the tube with and then completely wiping that tube down before you start any testing, so making sure that risk is mitigated. Or it’s controlled in the best way that you can before you move on to the next tasks. Next slide, please.
How about transportation? Now where will your testing be done for your specimens? How will you get them to that location?
We are strictly talking about if you are testing within your facility– so double bagging that specimen, putting it in a rigid container, making sure there’s absorbent material in case there is a leak. We recommend not using a pneumatic tube system with this. Pneumatic tube systems can break down– so just making sure that exactly where that specimen is going.
There’s many other considerations when you’re shipping or transporting outside of a facility that I’m not going to go into today. There’s lots of webinars that will discuss packaging and shipping. So this is strictly talking about how to get something from point A to point B in your facility, thinking through every single one of those steps and maybe looking at what is your route, how many people are on that route– so again, different things to think about. Next slide, please.
So other considerations– laboratory cleaning, disinfection, and some waste management. Waste management is always a big one on the list. The cleaning and disinfection, let’s talk about that first. Make sure that you have an EPA-registered, hospital grade disinfectant. The EPA’S website provides a list of disinfectants that are approved for Ebola.
And what you use may depend on your facility and what is available. However, be mindful of what you can and cannot use on your instrumentation as well as the contact time for that specific disinfectant that you’re using. Contact times vary based on the disinfectant used.
All right, waste management– while you are caring for your PUI, you may want to sequester your laboratory waste until the patient is either ruled in or ruled out. If they are ruled in as having Ebola, then that waste is now considered category A waste. Then the waste is highly regulated and will need to be handled according to federal, state, and local regulations.
You may want to create a log of specimens, including waste tubes, so that you know exactly where everything is in case that patient is ruled in or is a presumptive positive for Ebola. You want to make sure that the tubes do not end up accidentally somewhere else in the laboratory. We want to make sure that everybody is safe in this situation. Next slide, please.
You may also want to consider including the laboratory in your post-testing health care worker medical surveillance. If your patient is positive or presumptive positive for Ebola or whatever the pathogen of concern may be, you should consider setting up a monitoring process and including the laboratory personnel in that. Coordinate with your public health department on this.
So be honest with yourself. Listen to your body. If you are not feeling well, keep yourself and everyone around yourself safe. And let someone know, whomever that may be according to your facility’s policy, whether that’s leadership or whether that’s calling directly to your public health department. But we want to make sure that everybody is safe in this situation. Next slide, please.
So let’s move to administrative controls. Next slide, please. Now that you’ve identified the risks, you’ve determined how to mitigate those risks. You need to let your staff know this information. And we do this through writing specific operating procedures, doing trainings, making checklists to make it easier for staff.
And checklists can include what you may have ready for a patient when they come in. It could include a whole activation checklist, phone lists of people you need to call, staffing protocols, schedules, and things like that. Protocols could include cleaning and disinfection, how you’re going to do a spill cleanup, or et cetera.
Having these things in place once you’ve identified those risks and you’ve figured out how to mitigate those risks are going to help inform your staff on how to do everything and keep them safe as well. Training is a big one on this list. We want to make sure that your staff is trained through this, and they are comfortable, and that you’ve reviewed those processes, and that you don’t need to make changes to those processes. Next slide, please.
All right, so after you’ve done your risk assessment, you went through identifying and mitigating those risks. What tests are you actually able to do safely? Each facility may have a different answer on this based on their size, the resourcing, staffing, et cetera.
You’ve done your risk assessment. And you’re still finding that some of your processes are still in the high risk or extreme category. Then maybe your answer is that you can’t do this test. Remember, we want to make sure that your patient gets the best care possible. But your safety is just as important as the patient’s.
So if you’re unable to provide some of those routine tests for a viral hemorrhagic patient for whatever the reason may be– you don’t have the point of care instrumentation available. You can’t appropriately mitigate the risks. You don’t have a biosafety cabinet.
You don’t have other things. You don’t have funding to implement the controls needed. Or whatever that issue may be, then I would suggest reaching out to your public health department and discussing what your options would be.
Knowing your test capabilities will help them determine the best course of action. Maybe your health department could do some of the tests for you such as a malaria smear. Or perhaps they can discuss which facilities may be closest to you that could take your patient and provide more care.
The options of sending on testing to a different facility may be extremely limited. So again, we want to have those communications with your public health department, your leadership, whoever you need to talk to in order to communicate your capabilities and ensure that the patient care is not delayed. Next slide, please.
All right. Next slide, please. There are many resources that we’ve talked about. Here are some of them. We’ll have those available for you after the talk is over. Next slide, please.
And finally, I want to leave you with– there are lots of questions. There are lots of scenarios that I could have talked about today. I know there’s probably way more questions than I certainly could have answered today. But I just want you to know that CDC and NETEC are here to help you. We have much more knowledge than we had back in 2014.
So if you find yourself with more questions, please reach out to us. You can send questions to info@netec.org. We have a few NETEC laboratory subject matter experts.
And we would be happy to get back to you with some of your questions. Again, in the beginning, we talked about some of the ways that NETEC can help you. And we would all be happy to help with anything that you need.
Again, laboratory safety is one of my things that are close to my heart. And I want to make sure that all the laboratorians are as safe as they can possibly be. So next slide, please.
And you can follow NETEC. You can contact us online. You can follow all of the things that we are doing on the different social media platforms. We do have webinars as well. We do have resources available in our libraries. Next slide, please.
And with that, I have ended a little bit early. So I’ve given you guys a little extra time for your Q&A and happy to answer any questions that you guys have.
NANCY CORNISH: Thank you, Vicki. We do have some questions online. And I’m not sure which one we should answer first. I think we have one from Keith Irons.
“We were told that if an Ebola patient comes into our ER, then we have to evacuate and close down the entire ER and lock everyone in. Is this correct?” Would you like to answer that? Or would you like me to answer that?
VICKI HERRERA: Well, I’ll give you my take on that, Nancy. And then I’ll let you give [INAUDIBLE] as well. So again, we know a lot more things than we did in 2014. We know that there are ways to safely isolate without having to shut everything down.
But these are also conversations that you need to have with upper leadership. They need to have their fears and anxieties relieved. And part of what is going to help with that is clear communication and clear plans before you get a patient.
So again, there’s a lot more discussions that we can have on that. But again, communication is just key to that. Nancy, I’ll let you, if there’s more you want to add to that, go ahead.
NANCY CORNISH: Yes, I would like to point out that you will not know it’s an Ebola patient. You will know that you have a sick patient. You will not know that they have Ebola right at that moment.
I want to reinforce what Vicki said. You need to have a plan before that happens. And be ready for it, so working with your public health department– also working with your public health lab. So I think sometimes, it is very effective to call your public health lab and discuss some of these issues with them as well as your hospital administration.
So you need an emergency plan for any very sick patient that walks into the hospital. It might not be Ebola. It could be something else. So that’s, I think, what you need to do.
BRIAN HARCOURT: This is Brian. May chime in?
NANCY CORNISH: Absolutely.
BRIAN HARCOURT: Yeah, so not an MD– more of a lab guy. But I think for anything here, the biggest way you combat the fear is knowledge. So learn about, how is Ebola transmitted? If you don’t have any wet symptoms, it is very difficult to transmit it from one person to another, especially early on. Remember, if you do not yet have symptoms, you are not contagious.
Actually, the virus isn’t even detectable yet, the virus kinetics. And so the viremia isn’t up high enough to even detect until you’re symptomatic. One thing to consider, the gentleman in 2014 that came from Liberia who was in the hospital in Dallas, he lived with several people in his apartment. And none of them got Ebola even though he had some pretty wet symptoms.
So essentially, if you can stay away from vomit, diarrhea, blood, anything else, your chances of getting it are extraordinarily small. This is not spread by aerosols or anything like that, not like COVID. So if you sit, a guy, you sit next to an airplane with somebody who has Ebola, you’re not going to get it if you don’t come in contact with the body fluids.
So you remember that when you’re thinking about Ebola. Ebola has an astronomical fear factor. But if you can break it down to its components, and learn more about it, and remember your bloodborne pathogens and everything you’ve been taught about infectious diseases, that will really help you combat the fear and figure out the right thing to do. Over.
NANCY CORNISH: Yes, Brian. I appreciate that– also wanted to point out that the Texas patient went to the ED with symptoms. No one in the ED got sick. He was then sent back home.
He came back to the ED and then was finally admitted. But no one got sick. And I also want to point out that nobody in the laboratory got Ebola either even though they were handling all of his specimens.
BRIAN HARCOURT: Thank you. I had forgotten about he had gone to the ED. That’s a good point.
NANCY CORNISH: Yeah, twice.
BRIAN HARCOURT: Wow. [INAUDIBLE] wow.
NANCY CORNISH: Yeah. So yeah, I think the key here is to have a plan ahead of time. And I think that’s what we all need to work on. And that’s what we’re trying to help out with here.
VICKI HERRERA: And I’m just going to add to that. Again, NETEC has a lot of resources for identifying, isolating, and then informing people. So that is kind of your three key things to do if you have somebody that walks in with symptoms and you don’t know what they have.
NANCY CORNISH: Thanks. OK. So I’m looking here for some other questions. I think there was a question about malaria and where they could find a malaria protocol. So Brian Harcourt and I and the malaria branch are working on this. Brian, do you want to speak to that?
BRIAN HARCOURT: Sure, yeah. I think the language you came up with is going through final clearance.
NANCY CORNISH: Yeah.
BRIAN HARCOURT: But the bottom line is– and Nancy, why don’t you chime in on the thick smears? Because you had the idea. Then I’ll mention the thin smears.
NANCY CORNISH: OK.
BRIAN HARCOURT: So in 2014– and then, actually, 2016 as well– there was a paper published in Canada where they looked at modifying the thin smear protocol to have been able to inactivate Ebola. Or basically, it would inactivate any VHF. And what they did was, they extended the time of the methanol fixation, the 100% methanol fixation step, from a few minutes to 15 to 30 minutes.
And what we found in our lab– and then what the Canadians found in their lab and published it– it’s [INAUDIBLE] 2016. I can’t remember the journal off the top of my head– that it would inactivate close to seven logs of Ebola in those 15 minutes. So you can do thin smears with the extended methanol fixation step.
And somebody in Nancy’s shop Kathy Grady– is that her name– as we were– she was actually duplicating the methods with slides that had malaria pathogens in it. And it did not adversely affect her ability to read the slides. And then Nancy, if you want to speak about the thick smears–
NANCY CORNISH: Yeah, so thin smears, the Ebola can be inactivated by the extended methanol. Thick smears, that is not the case. So what we are recommending is, you could put a cover slip over it with a quickly drying mounting media. And so you could also do that with your thin smears if you felt that you wanted an extra layer of protection.
But the Ebola will not jump off the slide at you. It’s bloodborne. It’s not aerosolized. And once that slide is made and cover slipped, you have mitigated the risk. And I would also handle it with gloves.
VICKI HERRERA: So I just want to add to that, too. So again, with slides, you are dealing with sharps. The slides are sharp. So if you are looking at a PUI, make sure that you evaluate the appropriate PPE.
If you have the option to do those slides in a biosafety cabinet, that’s going to add a layer of protection for you. And just critically think through every step and how you can mitigate those steps if that patient were to be positive. So look at your PPE.
Look at the sharps. Look at, like they said, the ways to fix them so that they can safely be read. So just, again, look at every step. And try to mitigate every step with the best that you have available.
BRIAN HARCOURT: I guess, then, one last thing is if– don’t try to dry the slide with anything that produces a breeze like a fan or a blower. Because then you will more than likely produce fomites.
NANCY CORNISH: Right. And remember that whenever you’re looking at blood or working with blood, that patient could have other infectious diseases. So you need to be careful at all times. So it may not be Ebola. It may be something else you do not want to get. So be careful at all times– universal precautions, blood borne precautions.
So we have another question. “Are you aware of any instrumentation where vendors will not service it if we use the instrument for Ebola testing?” Now this was an issue in 2014. I have not heard of– I’ve heard that people are concerned about this.
But I have not heard about any manufacturers who say that they will not do it in 2022. So if you talk to your instrumentation representatives and they’re telling you that, if you would let us know which manufacturer it is, we can address that with AdvaMed, who represents manufacturers, and with ACLA, who represents clinical laboratories.
So we are in the process of discussing, and working out, and making a plan before anything happens with the manufacturers. Vicki– go ahead.
BRIAN HARCOURT: Yeah, and I’m helping to think these through. And this obviously is an extremely complicated question. Because one is just the broad scope of manufacturers and type of designs of instruments. But– and I don’t want this question to come across as snarky. That’s not the intention.
But it’s more of a thought experiment is, do you do this after you have an HIV positive patient or somebody dies of some horrible encephalitis of an unknown etiology? Do you clean your machines? Do you think about it? So again, this is kind of the fear factor taking over a little bit. I obviously respect it.
But think it through. And ask yourself, what do you do in those cases? I honestly don’t know what you do. Because that’s not my forte. I’m just trying to give food for thought kind of things to think through.
And so there are some instruments that are– some of the analyzers were kind of like flow cytometer that are closed systems that companies do have means for you to, if it’s a closed system with tubing, you can run bleach or whatever. All of them– a lot of them seem to have their own little proprietary solution to run through that can be disinfecting. So again, contact the manufacturers. That’s about the best thing I can say. Over.
NANCY CORNISH: Vicki, do you have anything to add to that?
VICKI HERRERA: Again, kind of what you guys have said, it’s going to depend on the manufacturer. There is such a broad list of manufacturers that I honestly do not know what each manufacturer is currently recommending. But just keep in mind that the infectious dose of Ebola is very small. So some things that you would normally put on an instrument, maybe this isn’t one of them– but again, just critically thinking through all of those steps and how you can mitigate.
NANCY CORNISH: Right, and I think that’s part of the plan to be ready for this would be to call your manufacturer’s representative and find out what they have to say about it. And contact us if they say that you can’t use the instrument anymore. And we will work with them.
VICKI HERRERA: Absolutely. Again, if you have questions, like Nancy said, reach out to her. Or reach out to NETEC. And we’d be happy to walk you through some things.
NANCY CORNISH: So there’s another question here. “Are there any instances where lab personnel are infected with viral hemorrhagic fever through open vial testing on a chemistry analyzer?”
VICKI HERRERA: So I am not aware of any in the United States. But what I also want to say is that our n for patients in the United States has been very low. So I think you have to look at every step, again, in your system.
Normally, we would recommend not using open tube systems. But again, there may be some ways that you could mitigate, whether that’s removing the testing personnel from the area– minimizing that– or wearing appropriate PPE. Do you have PAPR on hand?
Do you have N95s? Do you have mucous membranes all covered? So there may be some ways to mitigate that. But you really do need to think through every single step.
NANCY CORNISH: Brian, do you have anything to add to that?
BRIAN HARCOURT: I was searching for an answer to that very question the other day. I couldn’t find anything. Then I put my LLS fellow on it to see if she could. But I haven’t heard that she’s found anything either. Over.
NANCY CORNISH: Yeah, and we also looked and did not see any reported cases. So I think we have time for maybe one more question. “Our hospital wants to test in the same room as the patient and no hood in the room with POC instruments. You did not mention this option.” Vicki, do you want to take that since you guys have experience with this?
VICKI HERRERA: Sure. So it can be done. Just, again, keep in mind your risks if you can separate yourself as much from the patient as possible. But you also want to make sure you consider the PPE that you’re using since you will be in the patient room. And cleaning up, making sure that your laboratory supplies are sequestered as well.
So it is an option. Again, you just have to walk through what that means for being in the room with the patient and making sure that you have possibly another person, whether that’s the nurse in the room just available in case you need something. We still recommend that second person.
NANCY CORNISH: Thank you. If you have any questions after today, please feel free to email the OneLab™ inbox. And we will answer them. Alicia, you’re on.
ALICIA BRANCH: Thanks again to the NETEC presenters and CDC moderators for a great webinar today. I would like to highlight our next OneLab™ Network event, which is December 16 from 1:00 PM to 2:00 PM Eastern Standard Time. And it’s “Building a Laboratory Onboarding Template.”
It’s a fully customizable template for laboratory managers and staff who want to provide their new and [INAUDIBLE] staff with a centralized orientation manual for SOPs, where it’s your spill response information– all can be provided into this actual one resource. And we will actually guide each of the participants through using the laboratory onboarding template.
So to register for this event, the link has been posted in our chat. And remember, the slides with the links from today’s presentation will be available at cdc.gov/onelab within the next two weeks. And thanks again for joining. Have a great rest of your day. And a happy Thanksgiving to everyone.
BRIAN HARCOURT: Thank you. Happy Thanksgiving to y’all.
ALICIA BRANCH: Yeah.